Kidney stones are a multifactorial disease, and among the modifiable factors we can highlight: Lifestyle, Medications and Supplements, and Nutrients and Antinutrients.
There is growing evidence that nephrolithiasis is a systemic disease, as considerable links have been found between kidney stones and conditions such as hypertension, obesity, dyslipidemia, and insulin resistance.
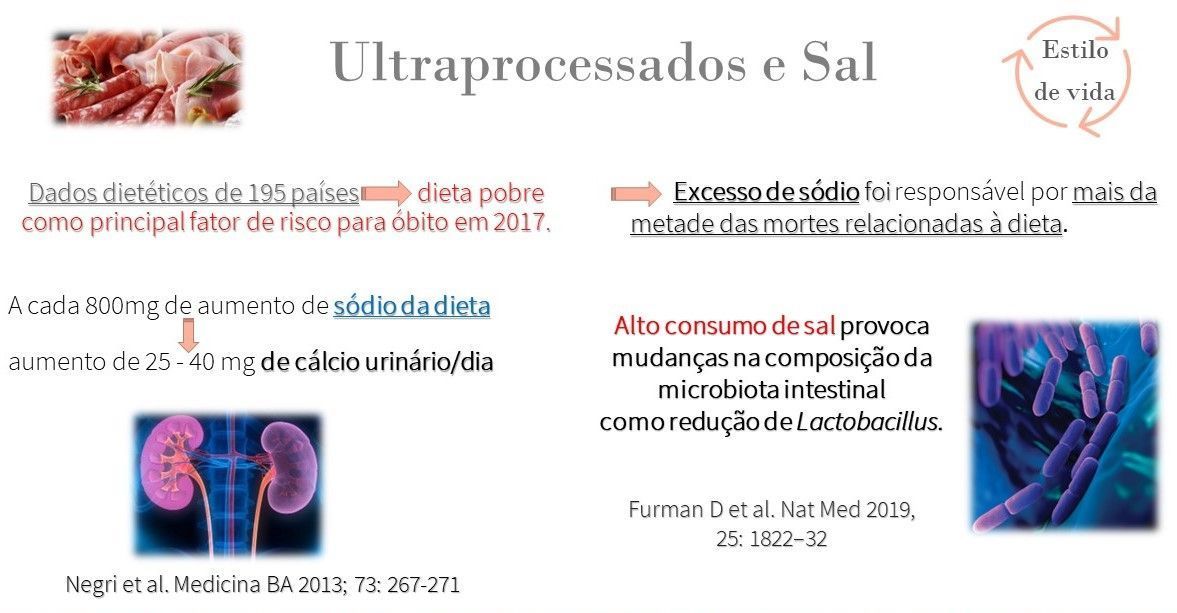
High sodium intake is primarily linked to the consumption of processed and ultra-processed foods. This consumption increases urinary calcium excretion, blood pressure, and harms the intestinal flora, variables closely related to the formation of kidney stones.
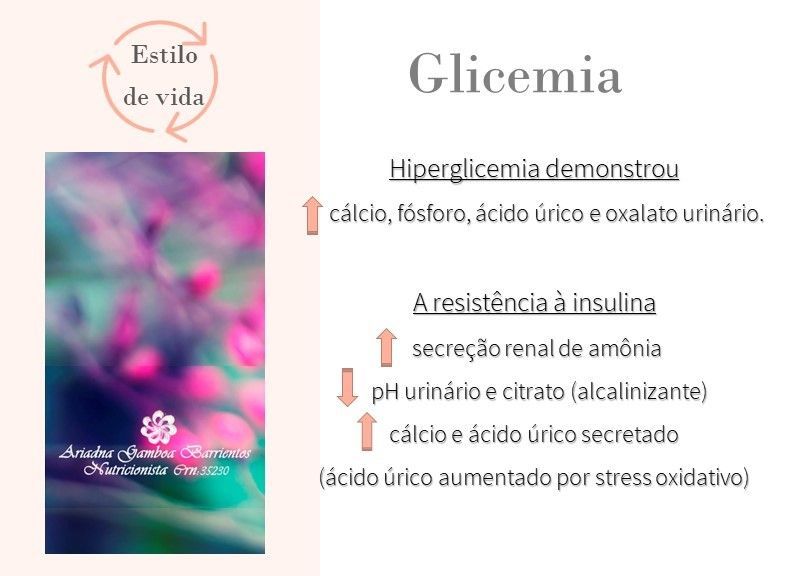
Changes in blood glucose levels and insulin resistance can also alter the urinary excretion of metabolites related to stone formation, changing urinary pH and increasing oxidative stress.
Regardless of the underlying cause of the stones, one of the cornerstones of conservative treatment is increasing fluid intake to achieve a daily urine output of 2 liters.
Moderate dietary salt restriction is useful for limiting urinary calcium excretion and therefore may be helpful in the primary and secondary prevention of nephrolithiasis. Several human studies have suggested that diets with higher intake of vegetables and fruits play a role in preventing kidney stones.
Low or normal protein intake reduces calciuria (calcium in the urine) and may be helpful in preventing kidney stones and preserving bone mass.
A diet rich in calcium (1200 mg/day) is helpful for maintaining bone health and preventing kidney stones, although higher supplementation may involve an increased risk of both kidney stone formation and cardiovascular disease.
A lower intake of animal protein combined with a higher intake of plant-based products reduces the acid load and uric acid excretion.
Medications associated with the formation of kidney stones:
Allopurinol, laxatives, loop diuretics, antacids, corticosteroids, theophylline, aspirin, topiramate, indinavir, triamterene, sotalol, amiodarone, antibiotics (sulfonamides, ceftriaxone, amoxicillin), and chemotherapy.
Vitamin C
Taking 1 to 2 g per day may increase urinary oxalate and the risk of calcium oxalate stones. According to studies, men, in particular, who are prone to forming calcium oxalate stones should avoid these supplements.
Calcium
According to a large study (Nurses Health), calcium supplementation can increase the risk of kidney stones by 20%.
And note: it's not just calcium supplements that contain added calcium! Many products like powdered milk or plant-based milks contain high amounts of calcium carbonate!!!
A study of 36,000 postmenopausal women found that supplementation with 500mg of calcium carbonate and 200 IU of vitamin D twice daily for 7 years increased the risk of kidney stones by 17%.
Vitamin D
This vitamin increases digestive absorption of calcium and urinary excretion of calcium, at least in the group of individuals prone to forming kidney stones.
Prospective studies: vitamin D alone or with calcium, and epidemiological studies with high doses of vitamin D, have found an increase in kidney stones.
The association between vitamin D supplements and the risk of kidney stones is not fully understood. However, the evidence, when combined, shows that vitamin D administration worsens the risk in patients predisposed to hypercalciuria.
In the long term, vitamin D supplementation increased the risk of hypercalciuria by 64%, but no difference was found in the calculations.
For calculations of:
Calcium oxalate
- Reduce protein intake (animal protein) to < 30% of total calories.
- Reduce sodium intake to < 2g/day
- Alkalize urine: drink citrus beverages, increase fruit, vegetables and legumes (magnesium and potassium) intake, and consume calcium >850mg/day.
- Restrict foods high in oxalates (>6mg): beetroot, spinach, chard, rhubarb, cocoa; limit vitamin C <1g/day (divide), supplement with B6.
See the oxalate table at the link >>
Calcium phosphate
- Reduce phosphaturia inducers: excess carbohydrates.
- Reduce dietary phosphate: dairy products, legumes, chocolate, and nuts (to one-third).
- Urine pH > 7 (acidify: cranberry juice, reduce citrus fruits)
Uric acid
- Relationship with Metabolic Syndrome, Insulin Resistance, Diabetes Mellitus
- Reduce protein intake (animal protein) to < 30% of total calories.
- Reduce or eliminate alcohol consumption.
- Alkalizing urine: citrus drinks, increasing consumption of fruits, vegetables and legumes (magnesium and potassium)
Sources:
Geraghty R, et al. BMJ Open 2020;10:e032094
Zhang Y et al. 2021, Plos One 16(4): e0250257.
Precious et al. Arch Italian Congress 2015; 87, 2
Higashijima et al. Seg Alim Nutr., 27: 1-16, 2020
Akhtar MS et al. Int J Food Prop, 14:1, 241-249, 2011
Bargagli M et al. Nutrients 2021, 13, 4363
J Bras Nephrol 2014;36(4):437-445
doi:10.1136/bmjopen-2019-032094
Hall et al, 2019, Cell Metabolism 30, 67-77
Negri et al. Medicina BA 2013;73:267-271
Ferraro et al. Am J Kidney Dis. 2016, 67(3): 400–407.
García M et al. Nutr Hosp 2019, 36(3):70-74
doi:10.1186/1475-2891-5-23
doi:10.1038/s41598-021-85723-3